It's a New Day in Public Health.
The Florida Department of Health works to protect, promote, and improve the health of all people in Florida through integrated state, county, and community efforts.
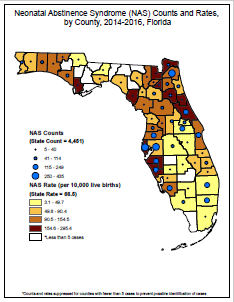
Surveillance of Neonatal Abstinence Syndrome (NAS) in Florida
Florida Birth Defects Registry
- 850-245-4405
- FBDR@flhealth.gov
-
Mailing Address
Division of Community Health Promotion, Public Health Research
4052 Bald Cypress Way
Tallahassee, FL 32399
Surveillance of Neonatal Abstinence Syndrome (NAS) in Florida
Neonatal abstinence syndrome (NAS) is a condition experienced by neonates exposed to opioid prescription or illicit drugs during the prenatal period. The infant may undergo withdrawal from these substances that manifests as excessive high-pitched crying, irritability, sleep-wake disturbances, alterations in infant tone and movement, feeding difficulties, or gastrointestinal disturbances, usually 1-3 days post-birth.
Recognizing the public health importance of the increasing trend in the prevalence of opioid prescription drug abuse and increasing incidence of NAS, the Florida Department of Health (DOH) added NAS to the List of Reportable Diseases/Conditions on June 4, 2014.
How are cases of NAS currently identified in Florida?
Data sources: To identify NAS cases, DOH currently uses a passive case ascertainment methodology that relies on linked administrative datasets and diagnostic codes indicative of NAS. First, birth certificate records from the DOH Bureau of Vital Statistics are linked to the infant’s birth hospitalization record, which is provided as part of quarterly submission of inpatient hospital discharge data by hospitals to the Agency for Health Care Administration (AHCA). Each discharge record includes International Classification of Diseases, Clinical Modification (ICD) diagnosis codes documented during the hospital encounter. The ICD classification system updated from ICD-9-CM to ICD-10-CM on October 1, 2015, impact all AHCA data beginning with the 4th quarter of 2015. The impact of this transition from ICD-9 to ICD-10 will need to be evaluated and addressed carefully during data acquisition, analysis, and interpretation of findings. Currently, there is no single ICD-9/10-CM code that captures NAS with sufficient sensitivity and specificity. Therefore, for NAS reporting, the following ICD-9/10-CM codes are being used as a proxy for NAS-related diagnoses:
ICD-9-CM | Thru 3rd Q 2015 | 779.5 | drug withdrawal syndrome in a newborn |
ICD-10-CM | 4th Q 2015 forward | P96.1 | drug withdrawal syndrome in infant of dependent mother |
Once an infant’s birth certificate record has been linked to his/her birth hospitalization, the discharge portion of the linked electronic record is scanned for the presence of any of the above-mentioned diagnosis codes.
What has been learned about the accuracy of the passive surveillance methodology and the data currently being analyzed to describe the prevalence of NAS in Florida?
In 2015, the Florida Birth Defects Registry (FBDR) conducted a statewide evaluation of the accuracy of ICD-9-CM codes that were used to identify potential cases of NAS. Findings suggested that ICD-9-CM codes 779.5 and 760.72 (narcotics affecting fetus or newborn via placenta or breast milk) had suboptimal accuracy in identifying infants with NAS. When verification of suspected NAS cases was based on a clinical definition proposed by a previous Epi-Aid investigation led by the Centers for Disease Control and Prevention (CDC), a substantial number of false positive cases of NAS were identified (i.e., had the 779.5 and/or 760.72 code, but did not meet the NAS case definition). Therefore, code 779.5 has been used to identify NAS cases prior to October 2015.
Considering the change from ICD-9-CM to ICD-10-CM beginning in October 2015, the FBDR is actively evaluating coding practices for the diagnosis of NAS cases beginning in October 2015. The primary issue is that there is not an exact translation from ICD-9-CM codes to the newer ICD-10-CM codes, and this lack of consistency could affect comparison of the rates that span the ICD-9-CM and ICD-10-CM coding eras. For example, what was captured by the 779.5 ICD-9-CM code as “drug withdrawal syndrome in newborn” (without distinction between maternal use of drugs versus from therapeutic use of drugs in the newborn) is captured in ICD-10-CM with better specificity. The FBDR is currently reviewing a small sample of 2016 NAS cases in order to describe ICD-10-CM coding practices using information gleaned from the medical record. Further active NAS surveillance is planned for 2017 NAS cases using a 20% sample that is representative of hospital- and patient-level characteristics statewide, which will facilitate case confirmation and analysis of NAS trends.
What are limitations of the data?
Currently, there appears to be substantial variation in the diagnosis and reporting of NAS across medical institutions, providers, and surveillance systems. These inconsistencies result in questionable accuracy and reliability of NAS data. However, they are also indicative of the need and opportunity for the DOH/FBDR to encourage establishment of a standardized set of recommendations and guidelines for clinical diagnosis, data collection, surveillance, and reporting efforts.
A limitation of using a passive surveillance methodology to identify NAS cases, particularly in the absence of case confirmation, is the likelihood for misclassification biases. These biases can result in both false negatives (the failure to capture an infant born with NAS) and false positives (identifying an infant as a NAS case does not meet the clinical definition of NAS). A second limitation is the timeliness of the data - the extent to which surveillance data are rapid, prompt, and responsive.
It is not yet fully understood how this ICD coding transition affected the observed frequency and rate of NAS, therefore changes in counts between 2015 and 2016 should be interpreted with caution. Moreover, there may be differences in coding practices across hospitals and regions, further impacting reported data. Because these data are linked to the discharge data, there are a percentage of cases that are missed and therefore the final numbers are likely an underestimation of the total counts. If the data were not linked to birth certificates, there would be an overestimation of the total counts. A decision was made to utilize the linked dataset for the final NAS counts in order to use similar methodology to other data utilized by the Florida Birth Defects Registry.
Despite these limitations, the use of an existing surveillance infrastructure with the capacity for efficient and effective review and confirmation of suspected cases will allow community leaders to respond to local concerns and provides insight into the epidemic of prescription drug abuse and its effects on babies.
Florida Neonatal Abstinence Syndrome (NAS) Methodology and Case Data:
NAS cases were identified from a linked data file comprised of AHCA administrative inpatient hospital discharge data and Florida birth certificate data from DOH Bureau of Vital Statistics for the 2014 and 2016 birth cohorts. The data are displayed by the birth quarter, and a * indicates that less than 5 cases were documented in a particular county for that time period.
DATA PARAMETERS
Florida Neonatal Abstinence Syndrome (NAS) Methodology and Case Data (continued):
- Patient is a Florida resident based on the patient state/county of residence reported on the birth certificate
- Diagnosis indicative of neonatal withdrawal symptoms based on a scan of the principal and up to 30 additional diagnosis codes present in the hospital discharge record*.
- ICD-9-CM code 779.5 was used in the 1st through 3rd quarter of 2015
- ICD-10-CM code P96.1 was used beginning in the 4th quarter of 2015
- Only included cases in which a NAS-related diagnosis code was documented during a hospitalization in which the age at admission was 28 days or less
- Linked birth certificates with AHCA hospital discharge data (current birth year and partial following year to also identify diagnoses for admissions the following year) to remove duplicates and preventing double-counting of NAS cases
- Excluded comprehensive rehabilitation discharges (e.g., a service type for a follow-up procedure other than birth) (type_serv variable not equal to 2 in the AHCA data file)
*For additional information regarding the specific codes used refer to the latest hopsital discharge data layout/dictionary, located at http://www.floridahealthfinder.gov/Researchers/OrderData/order-data.aspx

Connect with DOH